Introduction
The aim of the book, Why We Sleep, is to provide the general public access to a broad collection of sleep research. Below, I address thoughtful questions that have been raised regarding the book and its content in reviews, online forums and direct emails that I have received. Related, I very much appreciate being made aware of any errors in the book requiring revision. Furthermore, and as an essential part of what I see to be good scholarly conduct, I have made a full set of corrections to the book. These corrections have now been published in a second edition, which is now in print.
§ § §
Summary of points discussed below:
§ § §
Is sleeping 6 or fewer hours per night fine for your health?
A collection of experimental data does not support the assertion that 6 or fewer hours of sleep per night is sufficient for the optimal health of an average adult.
Below I describe a non-exhaustive set of studies that speak to this question, broken into three subsections: i) short sleep and the brain, ii) short sleep and the body, and iii) short sleep and genes.
i) Short sleep and the brain: An experiment by Van Dongen and Dinges and colleagues examined the following: what ‘dose’ of short sleep results in neurocognitive brain impairments?
They examined attentional lapses, otherwise known as microsleeps. This function of vigilant attention is a foundational element of numerous cognitive operations of the brain.
The study contained 4 different experimental groups. Each group was given a different amount of sleep.
One group was allowed 8 hours of sleep a night, a second group was limited to 6 hours a night, a third group 4 hours a night, and a fourth group was kept awake for 72 hours straight without sleep.
In the related figure, below, the vertical axis shows the number of neurocognitive lapses (microsleeps). The horizontal axis represents the time (number of days) in the study.
Noted in the cyan-coloured squares, after ~11 days of 6 hours of nightly sleep opportunity, participants were as neurocognitively impaired as those who had been sleep deprived (SD) for 24 hours straight (first horizontal dashed grey reference line in figure below [1]).
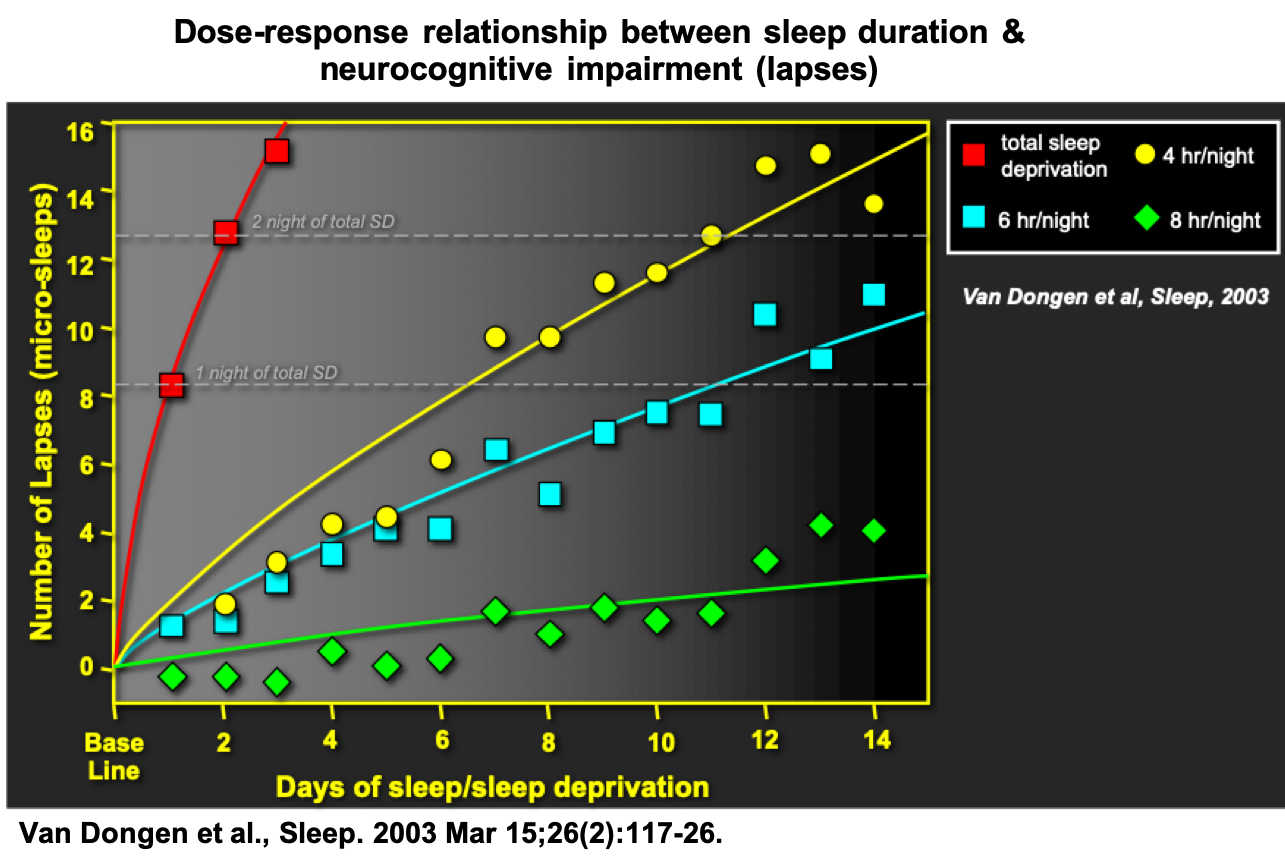
The conclusion of the researchers was that 6 hours of sleep is insufficient to support neurocognitive functioning of the human brain. They stated the following in their conclusion:
“Since chronic restriction of sleep to 6 h or less per night produced cognitive performance deficits equivalent to up to 2 nights of total sleep deprivation, it appears that even relatively moderate sleep restriction can seriously impair waking neurobehavioral functions in healthy adults.”
The scientists added a final sentence:
“Sleepiness ratings suggest that subjects were largely unaware of these increasing cognitive deficits, which may explain why the impact of chronic sleep restriction on waking cognitive functions is often assumed to be benign.”
Indeed, the authors calculated that the amount of sleep necessary to prevent neurocognitive impairment was 8.16 hours.
Consistent with this value, impairments in psychomotor performance (response times) have been reported in those limited to 7 hours of sleep a night for 1 week, relative to those provided with a 9-hour sleep opportunity.
These cognitive brain lapses, or microsleeps, have real-world consequences. Often, this is in the context of drowsy driving.
Supporting the above causal findings, a 2018 study evaluating over 3,000 individuals (men and women aged 40–89 years) reported the following: sleeping 6 hours a night was associated with a 33% increased risk of a car crash compared to those sleeping 7 or 8 hours a night.
Another approach to determining whether the brain has obtained sufficient sleep is to test for the presence of excessive sleepiness during the day.
Here, sleepiness reflects the neurophysiologic unmet need for sleep by the brain. Excessive daytime sleepiness is significantly associated with impairments in neurocognitive performance, described above.
To assess excessive daytime sleepiness, scientists and clinicians use the multiple sleep latency test. Participants are brought into a sleep laboratory during the day. The severity of excessive sleepiness is objectively measured by determining how likely it is that an individual will fall asleep, and how quickly.
Using this test, researchers examined a group of 632 adults (371 men, 261 women). They found a dose-response relationship.
Participants who slept fewer than 6.75 hours the night prior had a 73% increased risk of falling asleep during the day, compared to those who slept more than 7.5 hours.
Even those reporting between 6.75 to 7.5 hours sleep the night before had a 27% increased chance of falling asleep during the day, relative to those who obtained more than 7.5 hours of sleep.
These data indicate that sleeping 6 hours or less is inadequate for maintaining vigilant cognitive performance for an average adult. They further indicate that sleeping less than 7 hours is insufficient to meet the neurophysiological sleep need of the brain, as assessed by vulnerability to excessive daytime sleepiness.
ii) Short sleep and the body: Short sleep duration, and causal manipulations that restrict sleep, are associated with a significantly higher risk of numerous disease conditions and the development of disease features.
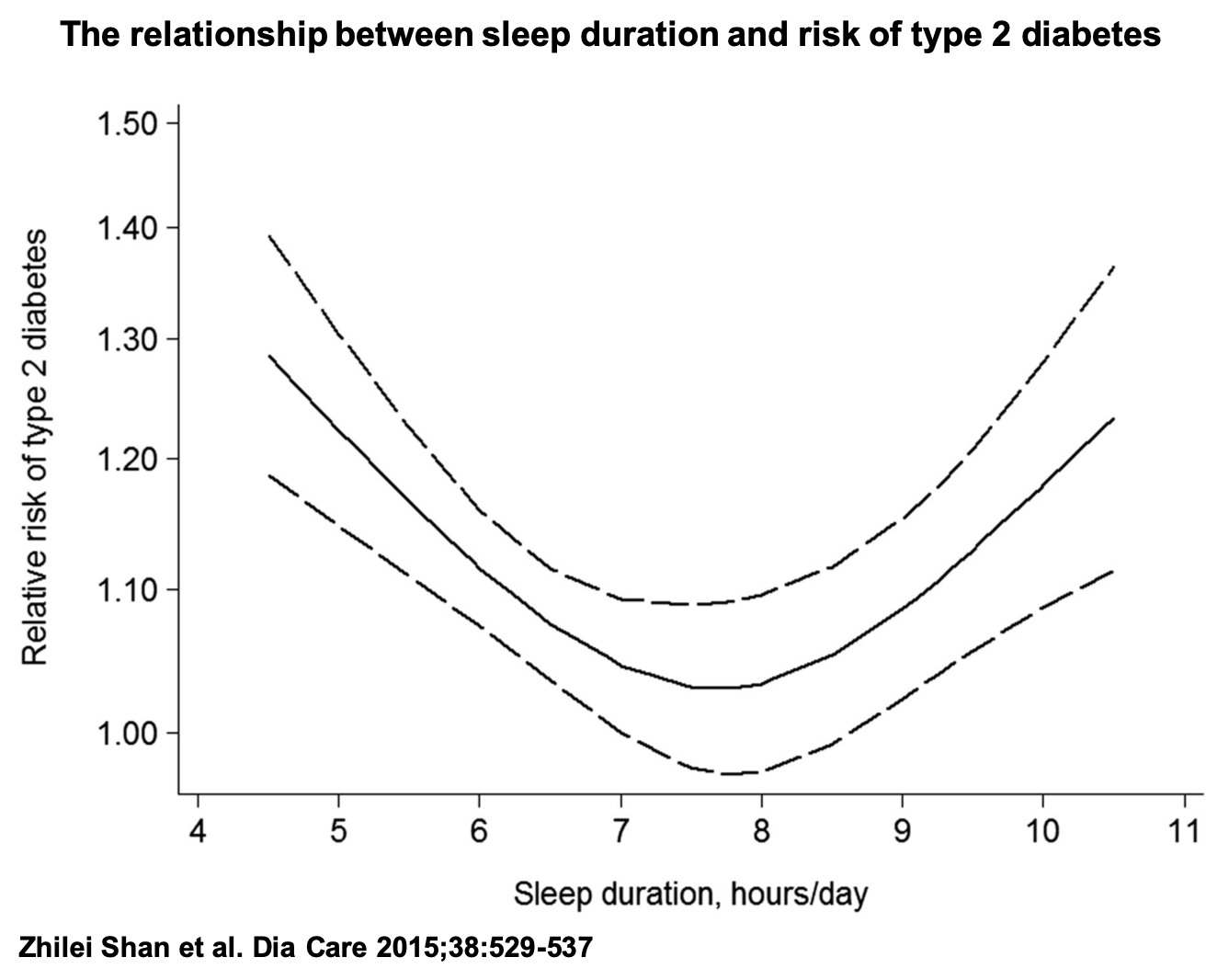
Type-2 diabetes is a condition involving impairments in insulin sensitivity leading to poor control of blood sugar (glucose).
A 2015 meta-analysis of prospective studies encompassing 482,502 participants observed a reverse-J/U-shaped function between sleep duration and risk of type-2 diabetes.
The lowest risk was observed at a sleep duration of 7-8 hours per day (figure, below). Relevant to the question of short sleep, an hour decrease in sleep was associated with a 9% increased risk of type-2 diabetes (with 7 hours of sleep per day as the reference).
Experimental studies in humans have now established the causal impact of short sleep on impaired insulin sensitivity. Summarized in a recent 2018 review, individuals restricted to short sleep (5.5 hours a night or less) suffered significant decreases in insulin sensitivity (figure below).
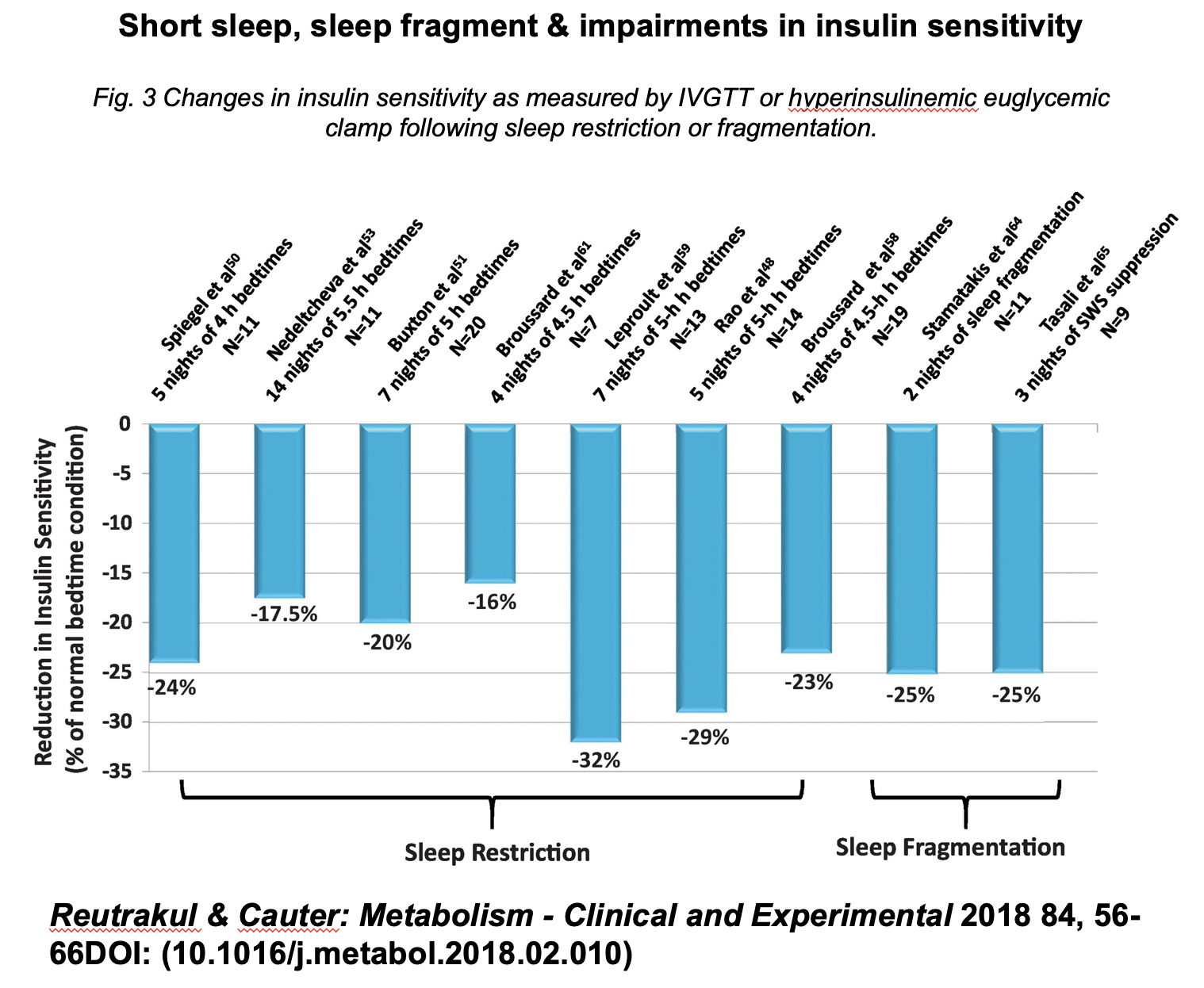
The conclusion of the authors was the following:
“Through well-designed experimental sleep manipulations, researchers have provided convincing evidence that insufficient sleep is a risk factor for obesity, insulin resistance and type 2 diabetes.”
Short sleep is also associated with a higher risk for cardiovascular disease (discussed in detail in the next section). Causal manipulations enforcing short sleep are now revealing the potential underlying mechanisms.
A 2014 study examined arterial vasodilation as a measure of blood-vessel (ill) health, also known as endothelial dysfunction: a recognized mediator of cardiovascular disease risk.
After 8 nights of 5.1 hours of average sleep, participants showed a significant impairment in arterial vasodilation relative to a control group averaging 6.9 hours sleep a night across 8 nights.
Based on this impact of short sleep on vascular function, the authors stated:
“The magnitude of impairment seen in this study with sleep restriction is similar to that reported in people who smoke, or have diabetes, or who have coronary artery disease, and helps further our understanding of the cardiovascular risk association with sleep deprivation.”
Similar vascular impairments have been reported in a randomized crossover study of healthy adults that compared a sleep-rested condition (>7 hours of sleep for 5 nights) with a short sleep condition (<5 hours of sleep for 5 nights).
In addition to the above vascular impairments, increases in (i) activity of the fight-or-flight branch of the nervous system (the sympathetic system), and (ii) an associated stress-related neurochemical, noradrenaline, also occurred under conditions of shortened sleep. Both of these latter features are themselves linked to cardiovascular disease.
Together, these data indicate that short sleep duration of less than 6 hours is insufficient for the optimal health of metabolic and cardiovascular systems.
iii) Short sleep and genes: Beyond the brain and physiological functions of the body, short sleep impacts the activity of genes.
A 2013 study examined the blood transcriptome in individuals limited to a 6-hour sleep opportunity for one week, relative to those same individuals when given a 10-hour sleep opportunity (during which they averaged 8.5 hours of sleep).
Over 700 genes were significantly altered in their expression following one week of short (6 hour/night) sleep. The altered genes included those controlling immune regulation, oxidative stress, inflammatory state, and metabolism.
The senior researcher of the study, Prof. Derk Jan Dijk, stated:
“Multiple epidemiological studies have shown self-reported short sleep duration – defined in most studies as less than 6 hours – is associated with negative health outcomes such as all-cause mortality, obesity, diabetes, cardiovascular disease and impaired vigilance and cognition.”
Commenting on the implications of the genetic alterations they discovered, he added:
“The identified biological processes may be involved with the negative effects of sleep loss on health and highlight the interrelatedness of sleep homeostasis, circadian rhythmicity and metabolism.”
Section Summary: Evidence does not support the assertion that obtaining 6 hours of sleep or less is sufficient for the health of an average adult [2].
§ § §
Is short sleep associated with a shorter life span (and is 9 hours of sleep or more too much)?
i) Short sleep and shorter lifespan: Chapter 12 of Why We Sleep described how both short and long sleep are associated with increased risk of mortality. The book stated the following:
Epidemiological evidence suggests that the relationship between sleep and mortality risk is not linear, such that the more and more sleep you get, the lower and lower your death risk (and vice versa). Rather, there is an upward hook in death risk once the average sleep amount passes nine hours, resulting in a tilted backward J shape.
The book further noted:
[it] is important not to overextend my point. I am not suggesting that sleeping eighteen or twenty-two hours each and every day, should that be physiologically possible, is more optimal than sleeping nine hours a day. Sleep is unlikely to operate in such a linear manner. Keep in mind that food, oxygen, and water are no different, and they, too, have a reverse-J-shape relationship with mortality risk. Eating to excess shortens life. Extreme hydration can lead to fatal increases in blood pressure associated with stroke or heart attack. Too much oxygen in the blood, known as hyperoxia, is toxic to cells, especially those of the brain.
Sleep, like food, water, and oxygen, may share this relationship with mortality risk when taken to extremes. After all, wakefulness in the correct amount is evolutionarily adaptive, as is sleep. Both sleep and wake provide synergistic and critical, though often different, survival advantages. There is an adaptive balance to be struck between wakefulness and sleep. In humans, that appears to be around sixteen hours of total wakefulness, and around eight hours of total sleep, for an average adult.
On this topic, a 2016 meta-analysis study published after the book was written has been cited as evidence of a U-shaped function of mortality risk linked to both short and long sleep. Interpretations have suggested that this paper supports the idea that short sleep is not associated with a shorter life, and/or that sleeping 5 to 6 hours a night is sufficient for health.
However, this was not the conclusion of the authors of this study, who stated the following about their findings:
“The results suggest that 7 hours/day of sleep duration should be recommended to prevent premature death among adults.”
There was no recommendation by the authors that sleeping 9 hours a night is inadvisable.
Given the presence of the U-shaped function in this study, it is necessary to add an additional comment regarding concerns about long sleep and mortality risk—a topic numerous readers have emailed me about (and is likely deserving of a dedicated essay all of its own).
First, the need for long sleep in some individuals can reflect poor quality sleep, which, in turn, can be associated with excessive daytime sleepiness. The latter can be indicated by a higher propensity for daytime napping.
Supporting this possibility, the link between long sleep duration and increased mortality was specifically observed among older women who reported being long sleepers but were taking daily daytime naps. This is indicative of daytime sleepiness linked to poor quality sleep.
In other words, mortality risk associated with long sleep—the far right side of the U curve—may, in part [3], reflect an association with poor-quality sleep, rather than too much sleep. This, together with issues of poor health and unmeasured comorbidities [4], as noted in the book.
Second, the measure of long sleep itself has been scrutinized. Based on the specific questions that various epidemiological surveys use, long sleep can be hard to differentiate from individuals simply reporting being in bed longer, rather than sleeping longer.
With that aside, and returning to the core question of this section—short sleep, there is another limitation of the above-cited 2016 study that has gone largely unmentioned in public discussion. The authors’ analyses relied on a measure of sleep that was taken many years before the critical assessment of mortality.
Said more simply, the study made assessments at two points in time. The first was the measure of sleep when participants entered the study. The second, taken later, measured mortality (whether the person was dead or alive). The problem is that these two measures were separated by a large amount of time—more than 20 years for some individuals.
The issue is this: the authors’ analysis had to assume that the amount of sleep a participant said they were getting when they entered the study remained exactly the same for the rest of their (studied) life.
For instance, if a woman reported sleeping 8 hours a night when they entered the study at age 55, the authors’ analysis assumed that they continued sleeping this same 8-hour amount each and every night until their death at the age of 75. This is unlikely for several reasons [5].
As a result, the analysis in the study cannot account for any changes in sleep in the participants. This impacts the confidence of the statistical model regarding an association between short sleep and mortality.
The inherent limitations of this study need to be appreciated when using it as a basis for an opinion on short sleep and mortality risk.
One approach to decreasing this inaccuracy is to reduce the study evaluation period between the first and second assessments. Related, a study of 4,713 participants examined death risk across a somewhat narrower time window of 9 years.
The authors identified the lowest mortality risk in individuals sleeping 7 or 8 hours a night. With that as a reference, the researchers found that men sleeping 6 hours or less had a 1.8 times greater age-adjusted death rate, and women a 1.6 times greater age-adjusted death rate. For long sleep (9 hours or more), the respective death rates were 1.4 and 1.5.
That is, short sleep of 6 hours or less was associated with a shorter life, compared to those sleeping 7-8 hours.
Another approach to limiting this inaccuracy is to measure an individual’s sleep duration several times over the study assessment period, rather than using a single initial baseline sleep measure.
Here, a study of 21,268 twins assessed sleep multiple times across the evaluation period. The lowest mortality risk was associated with those sleeping 7 to 8 hours.
Regarding short sleep, they found that sleeping less than 7 hours was associated with a significant increase in risk of mortality by 26% in men and by 21% in women.
Again, short sleep of less than 7 hours was associated with a shorter life, relative to those sleeping 7 to 8 hours.
NB: Discussed in detail below, to obtain 7 hours of sleep duration, an average healthy adult will need to be in bed for (i.e. have a sleep opportunity of) ~8 hours and 15 minutes.
ii) Short sleep and health span: Beyond considering mortality (life span), one must also consider morbidity in a discussion of short sleep. Morbidity contributes to an individual’s health span (how long they live without disease), in addition to their life span.
Short sleep has now been associated with a significantly higher risk of numerous disease states, including diabetes, poor immune-system health and cardiovascular disease.
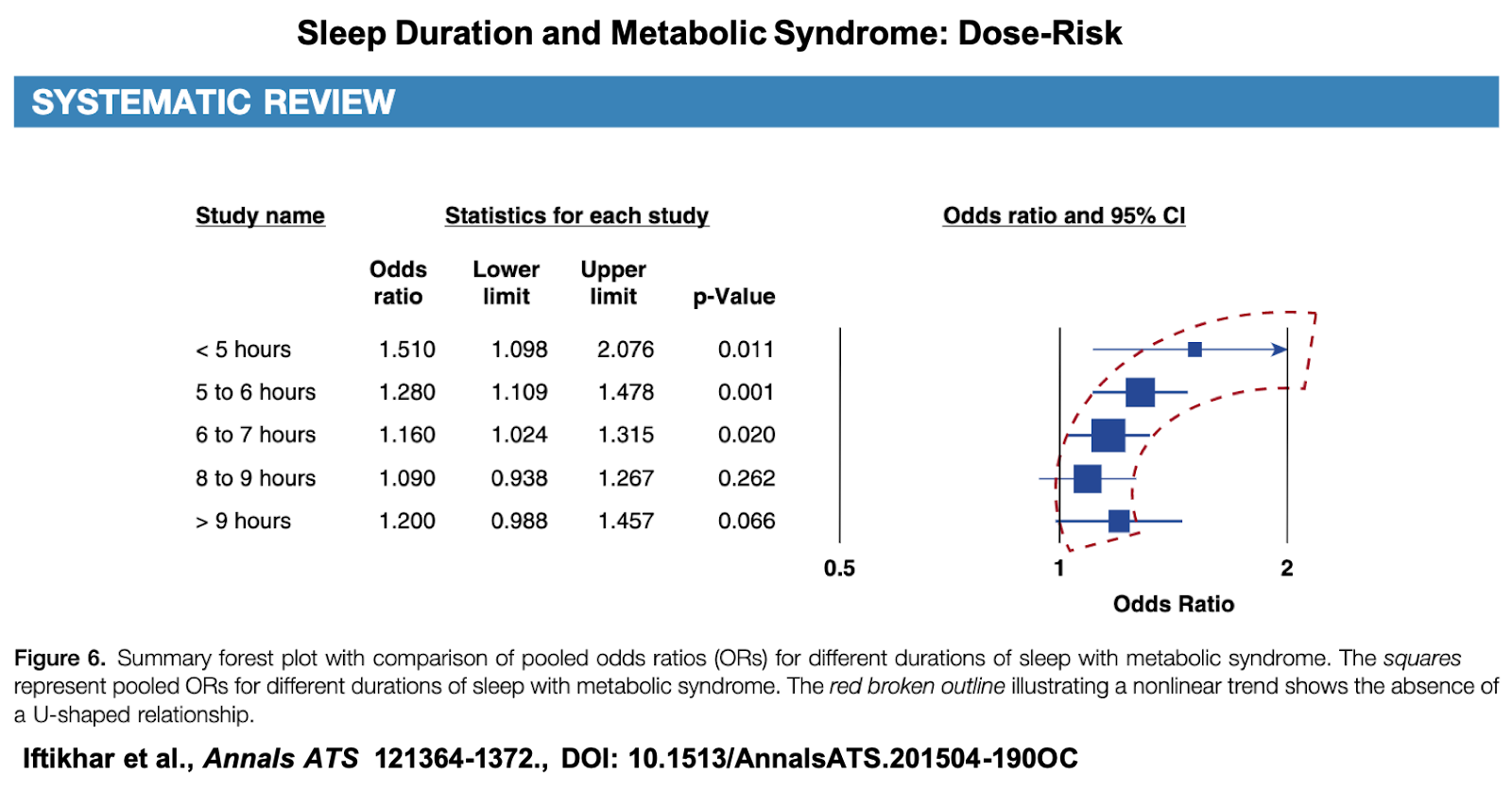
Examples include a recent meta-analysis of 75,657 people examining metabolic syndrome, a medical state that significantly increases a person’s risk of heart disease, stroke, and type-2 diabetes.
The meta-analysis demonstrated a reverse J-shaped association between sleep duration and the risk of metabolic syndrome (far right graph, blue squares in figure, below).
Relative to those sleeping 8-9 hours a night, a higher risk for metabolic syndrome was found for those sleeping 6-7 hours, 5-6 hours and <5 hours.
Turning to cardiovascular health, a 2019 study examined heart attack risk (myocardial infarction, MI) in one of the largest population samples to date—a total of 461,347 individuals in their main analyses.
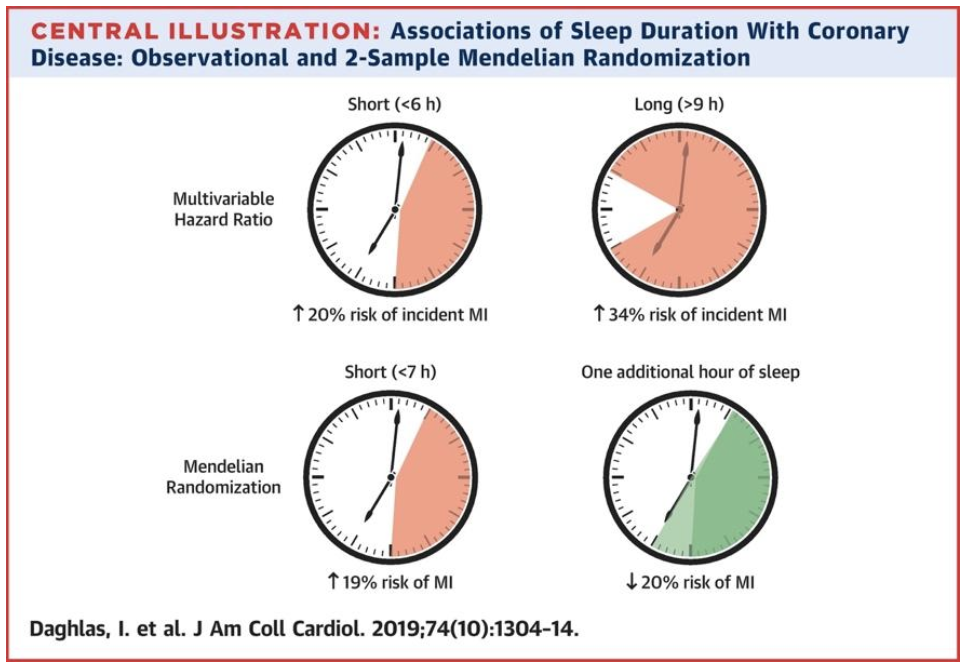
The researchers found that short sleep duration (those sleeping fewer than 6 hours) was associated with a 20% higher risk of heart attack incidence (hazard ratio, HR: 1.20).
Long sleep duration (those sleeping 9 hours or more) was associated with a 34% higher heart attack risk (HR: 1.34). Regarding any (mis)interpretation about long sleep duration, please see [6], the above commentary regarding what long sleep may reflect, and the below section discussing the concept of sleep opportunity.
Genetic analysis confirmed these results, showing that participants with a genetic predisposition for short sleep had an increased risk of myocardial infarction. Classifying participants based on genetics minimizes one of the major concerns with retrospective research, namely confounding variables. This approach is called Mendelian randomization. It allows scientists to make stronger inferences about causation.
Using Mendelian randomization, the authors were able to state:
“Prospective observational and MR [Mendelian randomization] analyses support short sleep duration as a potentially causal risk factor for myocardial infarction (MI).”
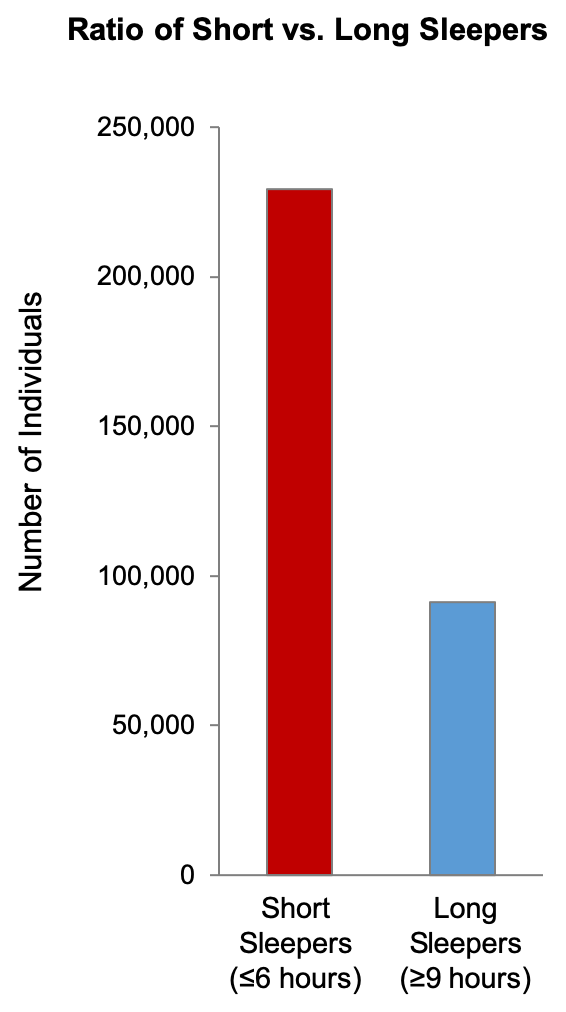
iii) The prevalence of short sleep: Returning to mortality, what is the respective prevalence of short versus long sleep in society? The question is relevant since it helps inform which of these two types represents a greater burden on/concern for society in terms of number.
Based on 17 studies [7] including a total of 837,452 individuals, there is a median 2.5 to 1 ratio of short sleepers vs. long sleepers (figure, below).
In other words, there are 2.5 times the number of short sleepers as there are long sleepers. This would suggest that the quantitative burden of short sleeping is 2.5 times greater than the burden of long sleeping.
Section Summary: Consistent with evidence stated in the book, both short sleep and long sleep are associated with increased mortality (life span) in epidemiological studies. This is also true for health span in the context of higher morbidity risks. Numerically, short sleeping represents a larger societal burden than long sleeping.
All epidemiological studies have limitations that must be appreciated, including those cited above. However, experimental studies have identified causal cellular, molecular and physiological mechanisms that help explain why short sleep may lead to these associated epidemiological risks (described in detail in Part II of Why We Sleep).
Yet, we do not have a similar set of demonstrated mechanisms explaining how long sleeping can be biologically harmful (and see [6]). Extant evidence suggests that long sleep duration can reflect the existence of unmeasured comorbidities and/or poor overall quality of sleep. Thus, it may be poor quality sleep and/or unmeasured health issues that are associated with higher mortality risk, rather than long sleep.
§ § §
What is the evolutionary relationship between reptiles, birds and mammals regarding sleep?
Chapter 4 of Why We Sleep addressed the evolution of sleep. Some readers have informed me that a section of this chapter could be interpreted as implying that birds and mammals commonly evolved from reptiles. Specifically, the book states:
However, insects, amphibians, fish, and most reptiles show no clear signs of REM sleep—the type associated with dreaming in humans. Only birds and mammals, which appeared later in the evolutionary timeline of the animal kingdom, have full-blown REM sleep.
Mammals and birds evolved from Synapsids and Reptiles, respectively. The latter two lineages are both descended from the common Amniote ancestor. This will be made clear in future editions of the book to prevent any confusion.
§ § §
Short sleep duration in males and associations with testosterone levels and testicular size.
In 2011, Leproult and Van Cauter demonstrated that young, healthy men limited to 5 hours of sleep a night for one week had a 10-15% drop in levels of testosterone, as well as associated reductions in vigor. Noted by the authors as a reference:
“By comparison, normal aging is associated with a decrease of testosterone levels by 1% to 2% per year.”
Thus, one week of short sleep in men (here, a 5-hour sleep restriction per night) resulted in levels of testosterone equivalent to those of someone approximately 10 years older.
Progressively shorter sleep duration is also associated with progressively lower levels of total and free testosterone in older adult males (figure, below, upper panel).
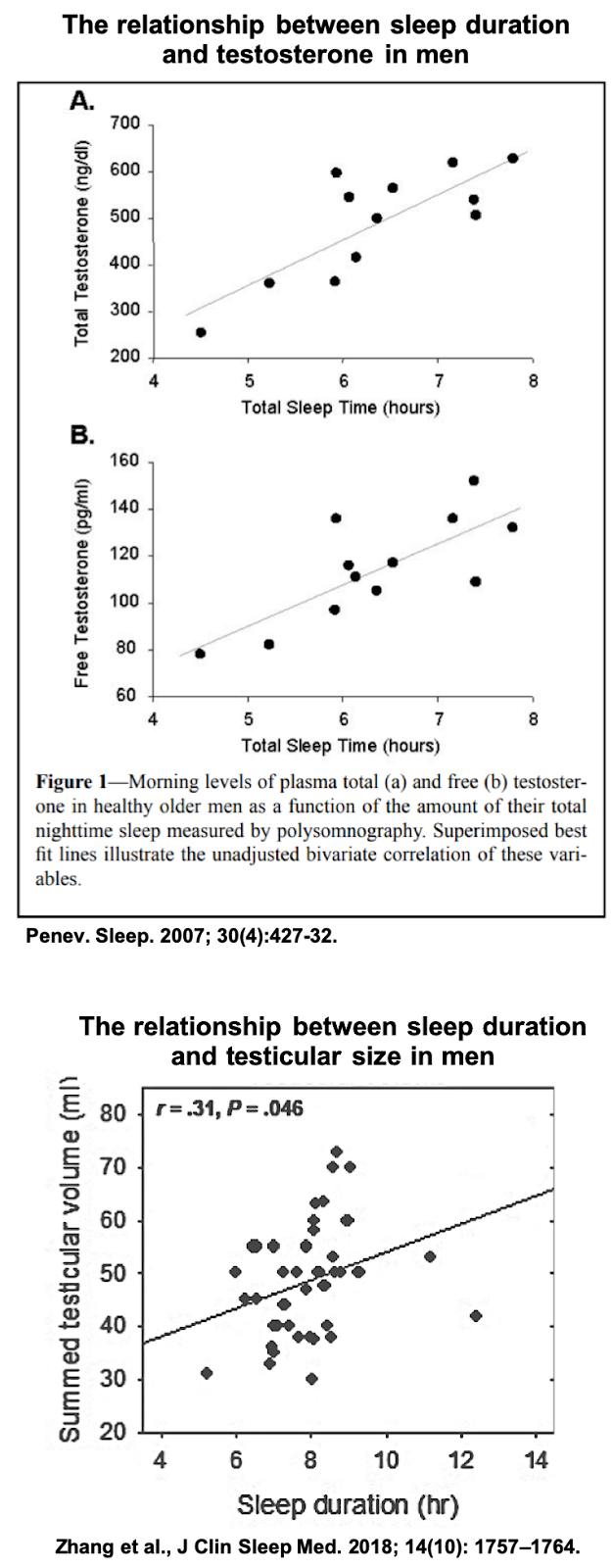
Fitting the above causal manipulation, experimental evidence in young men has further demonstrated that testosterone levels decrease with progressive time spent awake, yet increase across objectively measured time asleep.
Such data in humans is supported by causal sleep manipulations in animals, establishing that sleep loss significantly decreases serum testosterone. These changes do not appear to be restored following 4 days/nights of sleep recovery.
Finally, a 2018 study demonstrated that short sleep duration measured accurately using objective wristwatch actigraphy (rather than self-reported sleep) was significantly associated with smaller testicular volume (figure, above, lower panel).
Section Summary: Short sleep duration in males is associated with significantly lower levels of testosterone and reduced testicular size.
§ § §
Short sleep and the magnitude of associated cancer risk.
There are over 100 different types of cancer. Insufficient sleep is differentially associated with various types of cancer. Short sleep is by no means associated with a higher risk of all forms of cancer. Several studies, however, have indicated that short sleep is associated with a doubling of risk for specific cancers:
Described in a 2014 study, 2,586 men sleeping 6.5 hours a night or less had more than a two-fold greater risk of lung cancer after adjusting for smoking history (hazard ratio (HR): 2.12 [8]).
A study of 45,748 Japanese women assessed within a narrow follow-up period (median 7.6 years) demonstrated that sleeping less than 6 hours a night was specifically associated with a two-fold greater risk of ovarian cancer (odds ratio, OR: 2.00) relative to those sleeping 6-7 hours a night.
In a cohort of 173,327 men, short sleep was selectively associated with more than a two-fold greater risk of thyroid cancer (HR: 2.09) when comparing <5 hours vs. 7-8 hours of sleep.
In the same cohort, sleeping <5 hours vs. 7-8 hours was also associated with a more than two-fold greater risk of myeloma (HR: 2.06), a cancer of the blood linked with lymphoma and leukemia.
A meta-analysis published after the book was written, which examined 9 main forms of cancer (spanning a total of 20 subtype cancers), did not find an association between an all-cancer category and sleep duration.
While there is ready evidence associating certain cancers with short sleep, this study indicates that there are numerous cancers that do not show such an association. This will be reflected in future editions of the book. The revision to the book will also describe the limitations of the meta-analysis study, which are:
- Most of the included studies measured sleep at a single point in time, and often many years before the cancer assessment was made. As discussed above, the single-point assessment method prevents the study from being able to account for any changes in the sleep patterns of individuals over time.
- Subgroup analyses for different cancers were not equivalent in the amounts of data analyzed. That is, their sub-category analyses were not statistically robust enough (a.k.a. “powered”) to detect sleep duration effects.
- Finally, because only a select number of all cancers were assessed, the authors stated that their results “cannot be generalized to all cancer types.”
Importantly, epidemiological data cannot be used to inform causality. It is not correct to suggest, based on epidemiological findings, that sleeping less than 6 or 7 hours causes cancer.
However, one similarly cannot state that sleeping less than 6 hours a night does not double your risk of cancer. The same evidence cannot establish causality in the negative: absence of evidence in observational epidemiology does not necessarily imply evidence of absence.
Instead, it is randomized, controlled trials and experimental manipulations that can help inform causality, including the mechanisms underlying the association between insufficient sleep and cancer.
In this regard, a study by Dr. David Gozal and colleagues implementing a causal manipulation of sleep in mice is of note.
One group of mice had its sleep disrupted for several weeks, while a control group of mice was allowed to sleep normally. Both groups of mice were injected with tumor cells.
Linked to alterations in immune function, the tumors grew significantly faster and larger in the mice whose sleep was fragmented, relative to the mice allowed to sleep normally.
The tumor development was also more aggressive in the sleep-disrupted mice, spreading to other regions beyond the initial injection site—an indication of the cancer becoming metastatic.
Section Summary: Short sleep is associated with a higher risk of some, but by no means all, cancers. Causal manipulations in animal models are beginning to identify mechanisms that underlie the relationship between insufficient sleep and cancer.
§ § §
Is a lack of sleep deadly?
i) Fatal Familial Insomnia: Chapter 12 of the book considers the disorder of Fatal Familial Insomnia (FFI), for which there is no effective treatment or cure [9]. Readers have wondered whether the lack of sleep brought about by the condition is in fact fatal.
The book’s statements are fitting with the conclusions of a prominent 2008 review, which states:
“Prolonged sleep deprivation is also fatal in flies, cockroaches, and humans with fatal familial insomnia, who die after developing a syndrome not unlike that seen in sleep-deprived rats.”
Similarly, described by the National Organization of Rare Diseases and reflecting the given name of this medical disorder (i.e. denoting fatality), the organization states:
“The lack of sleep leads to physical and mental deterioration and the disease ultimately progresses to coma and death”
In their published discussion of FFI, Kaufman and colleagues also state the following:
“FFI follows a relentless fatal course over 6 to 36 months”
However, regarding sleep deprivation as the cause of death in FFI, the book was careful to state that:
“Scientifically, however, it remains arguably inconclusive, as there may be other disease-related processes that could contribute to death, and they are hard to distinguish from those of a lack of sleep.”
ii) Experimental sleep loss and death: That a lack of sleep rather than downstream consequences of sleep’s absence (e.g., neuronal cell death, immune system failure) leads to death in FFI has been debated, as noted above in the book. It has, however, been suggested that FFI was the only example provided in the book indicating that a lack of sleep may be lethal. Yet this is not the only evidence in the book that illustrates how a lack of sleep can lead to death.
Chapter 12 of the book described a series of studies in rats by Rechtschaffen, Everson and colleagues that addressed whether a lack of sleep is lethal.
These animal studies were included in the book because they offer an experimentally controlled test of this lethality thesis. Rechtschaffen et al., demonstrated the following three results:
1) Rats completely deprived of sleep died, on average, after 16 days in one experiment and 20.9 days in another. The authors concluded the following about the rats that had been deprived of sleep:
“Experimental [sleep deprived] rats suffered severe pathology and death; control rats did not.”
2) Rats who were selectively deprived of rapid eye movement (REM) sleep died within 27-54 days.
3) Rats who were selectively deprived of non-rapid eye movement (NREM) sleep died within 28-66 days.
Chapter 12 of the book went on to discuss earlier studies by de Manacéïne [10], describing how sleep deprivation was lethal in young dogs.
This study also compared sleep deprivation with the speed of death caused by total food deprivation. de Manacéïne concluded the following [11]:
“the total absence of sleep is more fatal for the animals than the total absence of food.”
Finally, in Chapter 12 of the book, I outlined similar studies by Italian researchers Tarozzi and Daddi [12]. They demonstrated that sleep deprivation caused death in adult dogs, and did so within 9-17 days [13].
These studies also reported that experimental sleep deprivation lead to neuronal (brain cell) death, a feature also observed in FFI patients.
It is important to acknowledge the issue of stress in some of these studies. The procedure of depriving an animal of sleep can be a stress itself. Thus, the stressful experimental procedure used to impose sleep deprivation may be what causes death, rather than the absence of sleep.
To control for this issue, the above studies in rats used what is called the “yoked control” method. Here, a control rat undergoes the same experimental stressor experience used for the sleep deprivation procedure, except it still has the opportunity to sleep near-normal amounts. These rats do not die, despite undergoing the same experimental stressor procedure as the sleep-deprived rats.
Section Summary: The data indicate that a specific lack of sleep can be deadly.
§ § §
Is acute sleep deprivation beneficial in the context of depression?
i) The benefit: Chapter 7 of Why We Sleep described how (and potentially why) a night of sleep deprivation is theraputically beneficial in 30-40% of patients with depression. In 2017, after the book was written, a meta-analysis of randomized treatment studies revised this antidepressant benefit response to 45% of patients. Future editions of the book will reflect this updated value.
My own lab has published neuroimaging findings supporting this clinical treatment approach, focused on reward centers of the brain. The data may illuminate some of the potential underlying mechanisms of the antidepressant benefit in these patients. Reflecting on these findings, and reinforcing this beneficial clinical effect, the book stated:
“Depression is not, as you may think, just about the excess presence of negative feelings. Major depression has as much to do with absence of positive emotions, a feature described as anhedonia: the inability to gain pleasure from normally pleasurable experiences, such as food, socializing, or sex. The one-third of depressed individuals who respond to sleep deprivation may therefore be those who experience the greater amplification within reward circuits of the brain that I described earlier, resulting in far stronger sensitivity to, and experiencing of, positive rewarding triggers following sleep deprivation.
That I would endorse a lack of sleep as beneficial for a set of patients with depression has been taken as being contradictory to my advice that a good night’s sleep is most beneficial in healthy adults. I do not see these two positions as contradictory, but rather accurately reflecting the scientific evidence on this matter—and its complexity.
ii) The constraints: Unfortunately, at present, there is a lower likelihood that sleep deprivation could be implemented as an everyday or unsupervised therapy for a number of reasons.
First, the antidepressant benefit of sleep deprivation typically and rapidly goes away following subsequent nights of recovery sleep. Implementing sleep deprivation or partial sleep deprivation can therefore be challenging as a treatment option. It is one of the reasons that such treatment is not widely used as a first-line therapeutic approach in major or bipolar depression, despite the fast-acting benefit.
The above 2017 meta-analysis study reflects this same conclusion. The authors stated:
“There has not been widespread adoption of sleep deprivation as a clinical treatment, however, because improvements are typically lost following a subsequent night of sleep. Indeed, research shows that greater than 80% of those who respond to sleep deprivation relapse following a night of sleep.”
Second, the practice of acute sleep deprivation for depressed patients should be done under clinical supervision, and not undertaken by the patient alone.
Third, insufficient sleep itself significantly increases the risk for depression, whether depression is measured as a clinical diagnosis, or in the form of depressive symptoms. Studies by John et al., 2005, Goodwin et al., 2008, Ryu et al., 2011, Fernandez-Mendoza et al., 2015, and Furihata et al., 2015 show a link between depression/depressive symptoms and short sleep, where the definition of short sleep ranges from 5-7 hours or less.
Moreover, in some patients, sleep-deprivation therapy, including multi-day sleep deprivation with the assistance of light therapy, has itself been associated with the triggering of anxiety attacks. This is consistent with recent causal evidence in healthy individuals demonstrating that both acute sleep deprivation and modest sleep restriction trigger anxiety and underlying changes in functional brain activity and brain connectivity.
Fourth, insufficient sleep is significantly associated with one of the most tragic components of major depressive disorder: suicide.
The first episodes of depression can often emerge in young adults and teens. In this group, Winsler et al. showed that progressively less sleep was associated with an increasing prevalence of suicidal features in a cohort of 27,939 adolescents (figure below, yellow and blue lines).
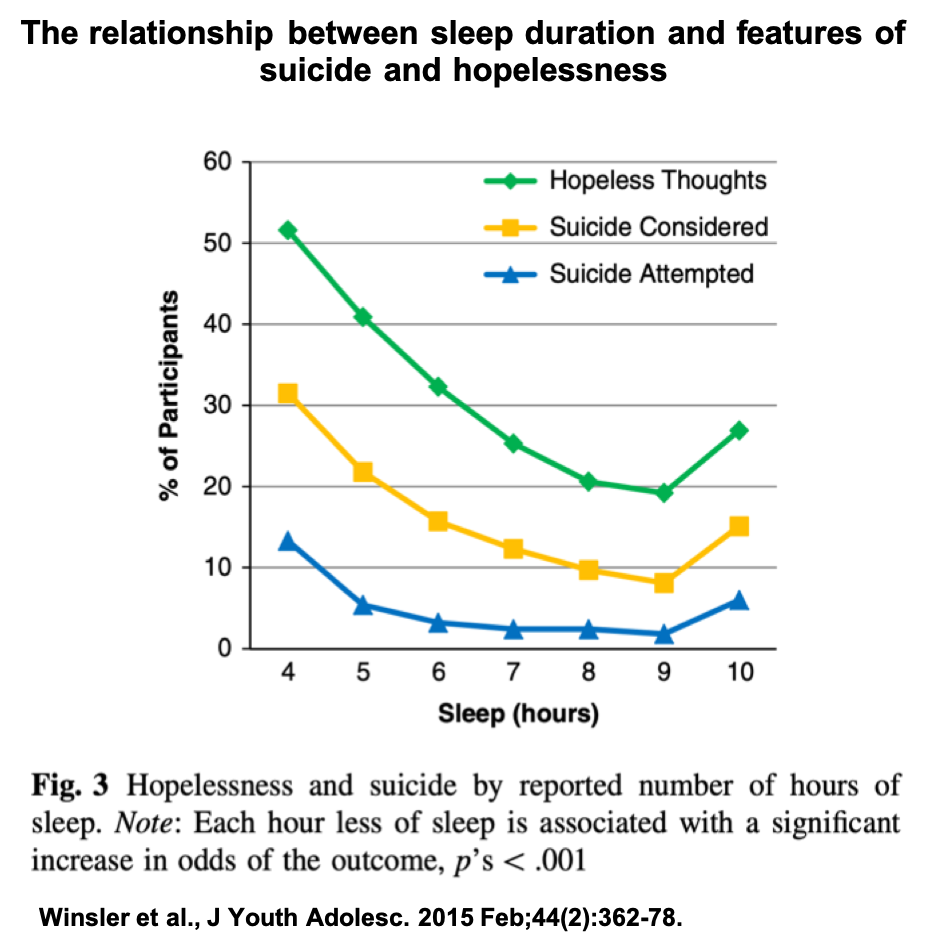
The lowest rates of these suicidal features were observed in those individuals who reported sleeping 9 hours a night.
Similar results were published by Rhie and Chae in 2013 in over a quarter of a million adolescents, demonstrating an association between short sleep and suicidal features. Sleep duration of 7-9 hours was associated with the lowest rates of suicidal measures.
Section Summary: Acute sleep deprivation can be beneficial as an antidepressant in 45% of patients with major depression. However, insufficient sleep is itself associated with an increased risk of depression and features of suicide.
§ § §
Are two-thirds of adults failing to obtain 8 hours of nightly sleep, and does sleep opportunity matter?
i) Are two-thirds of adults failing to obtain 8 hours of sleep a night, and the sleep they feel they need? The recommendation by the National Sleep Foundation is 7-9 hours sleep duration for healthy adults (ages 18-65). Fitting the mean of 8 hours of sleep, the Division of Sleep Medicine at Harvard Medical School states:
“What we do know is that sleeping fewer than about eight hours per night on a regular basis seems to increase the risk of developing a number of medical conditions.“
Data published by the Centers for Disease Control (CDC) show the following regarding the question of sleep time in US adults:
11.8% reported ≤5 hours,
23.0% reported 6 hours,
29.5% reported 7 hours,
27.7% reported 8 hours,
4.4% reported 9 hours,
3.6% reported ≥10 hours.
Thus, 64.3% of individuals reported sleeping less than 8 hours.
Results of a 2011 National Sleep Foundation poll align with these CDC values. The data demonstrate that almost two-thirds of US adults (63%) said their sleep needs were not being met during the week.
In addition, a 2013 National Sleep Foundation poll indicated that the average sleep amount of US adults during the working week is 6 hours 31 minutes.
Other developed nations reporting insufficient sleep included the United Kingdom, with an average of 6 hours and 49 minutes, and Japan, which reported an average of 6 hours and 22 minutes.
ii) Does sleep opportunity matter? The sleep recommendation given in Chapter 2 of Why We Sleep was the following (bold emphasis added):
In general, these un-refreshed feelings that compel a person to fall back asleep midmorning, or require the boosting of alertness with caffeine, are usually due to individuals not giving themselves adequate sleep opportunity time—at least eight or nine hours in bed.
Three metrics are important here. Sleep opportunity, sleep duration, and sleep efficiency.
Sleep opportunity: Total amount of time a person spends in bed.
Sleep duration: Total amount of time a person is asleep.
Sleep efficiency: The percentage of time a person is asleep (duration) relative to the total amount of time spent in bed (opportunity).
So, if you are in bed for 10 hours (sleep opportunity), and you sleep a total of 8 hours (sleep duration), you would have an 80% sleep efficiency.
In sleep research, a sleep efficiency of greater than 85% [14] is typically regarded as healthy. Why is this pertinent to the question of this section? Because sleep efficiency is different from sleep duration.
Let’s assume that every adult in the population has a healthy 85% sleep efficiency. We then realize that to obtain a minimum sleep duration of 7 hours, you require a sleep opportunity of 8 hours and 15 minutes in bed (reflected in the book’s description, above).
Indeed, the CDC is careful in its categorization of short sleep, defined as duration:
“Short sleep duration is defined as less than 7 hours of sleep per 24-hour period.”
Unfortunately, the reality is that not all people have a healthy sleep efficiency, especially in older age. Reported in a population meta-analysis by Carskadon and colleagues, on average, sleep efficiency drops below 85% by approximately age 60, and below 80% by age 80.
Thus, in order to maintain a minimum of 7 hours of sleep duration, a greater sleep opportunity is required in those with lower sleep efficiencies. Hence the book’s description of an 8- to 9-hour sleep opportunity that accommodates this nuance, and the innate variability in sleep need across average adults [15].
Section Summary: Survey data indicates that up to two thirds of adults in specific developed nations do not routinely obtain 8 hours of sleep duration a night.
§ § §
Does the number of vehicular accidents caused by drowsy driving exceed the combined number of vehicular accidents caused by alcohol and drugs?
The number of vehicle accidents in the United States associated with drowsy driving is considered to be between 70,000 and 1.2 million a year (see also NHTSA website).
Fatal vehicle accidents associated with drowsy driving are estimated to be around 15-20% (see also data from the AAA Foundation for Traffic Safety). However, where alcohol-consumption-related driving accidents are relatively easy to quantify, it is harder to prove whether a fatal accident is directly related to fatigue. Therefore, many researchers and policymakers believe there is an underestimation of the number of vehicle accidents caused by sleepy driving. A report from the National Transportation Safety Board states:
“Although generally accepted as a factor in transportation accidents, the exact number of accidents due to fatigue is difficult to determine and likely to be underestimated. The difficulty in determining the incidence of fatigue-related accidents is due, at least in part, to the difficulty in identifying fatigue as a causal or contributing factor in accidents.”
In 2009, the Report of the Special Commission on Drowsy Driving explained why safety administrations underestimate the number of drowsy-driving-related accidents. Based on firsthand data from cameras installed in cars, they stated:
“In 22% of all motor-vehicle crashes and 16% of all near crashes, the crash was directly attributed, at least in part to drowsiness, and a proportion far in excess of that suggested by police reports, and roughly equivalent to the proportion of crashes attributable to all other sources of distracted driving (such as cell phone use, eating, putting on makeup, etc.) combined. Moreover, since drowsiness can increase the propensity to become distracted and to intentionally employ distractions (e.g., talking on a cell phone, turning up the radio) as a means of staying awake, drowsiness may explain an even larger proportion of distracted driving crashes than those directly attributed to it.”
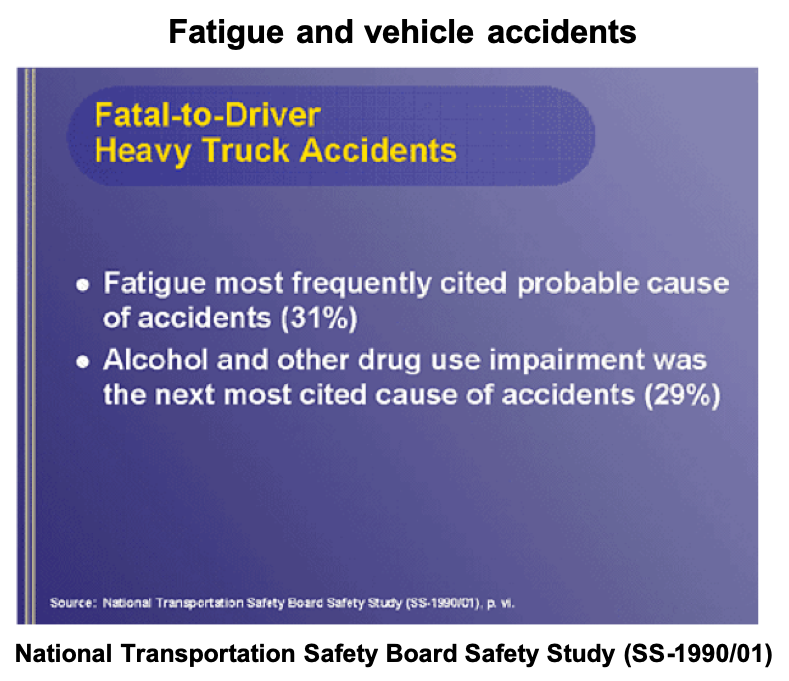
Additionally cited in the report (and see figure, below):
“Another relevant study, conducted in 1990 by the National Transportation Safety Board, examined 182 heavy truck crashes that were fatal to the driver. The study showed that 31% of the crashes in the sample involved fatigue – equal to fatal drug and alcohol-related crashes in the sample combined.”
Section Summary: Drowsy driving is a significant contributor to vehicle accidents and fatalities [16]. Indeed, leading transportation committees conclude that they most likely underestimate this number. For this reason, it is hard to objectively quantify the number of accidents and fatalities caused by drowsy driving relative to intoxicated driving. Revisions in the next edition of the book will note this point, and the above statistics.
§ § §
Associations between sleep and cardiovascular disease discussed in the book
One report discussed in Why We Sleep evaluated 7,428 Japanese employees, of which 4,652 were male. However, the number of males incorporated in the final analysis was 2,282. Thus, a revision to the book will note the important correction that the study cohort did include over 4,000 males, but that 2,282 were included in the final analysis.
In the study, cardiovascular events were classified as those including stroke and sudden cardiac death (i.e. sudden cardiac arrests). Coronary events were assessed separately, defined as myocardial infarction (i.e. heart attack) or angina pectoris, requiring coronary artery bypass grafting or catheter intervention.
Short sleep (less than 6 hours a night) was associated with a 3.2–3.6 times increased risk for cardiovascular events, and a 4.1–5.1 increased risk for coronary events. This was relative to those sleeping 7-7.9 hours a night.
Based on this, there are several corrections that are required in the book: (i) the specific cutoff for the sleep analysis amount (sleeping less than 6 hours, rather than 6 hours), (ii) the type of outcome associated with short sleep (cardiac events, rather than cardiac arrests) (iii) and their respective risk increase (defined as a times-greater risk, rather than an incorrect percentage).
Another study discussed in the book evaluated more than half a million individuals. However, based on the inclusion criteria, 474,684 participants were ultimately analyzed. This point necessitates correction in the book: the study analyzed almost half a million (474,684) individuals, not over half a million.
Additionally, the authors of this study reported that short sleep duration (typically ≤5–6 hours per night) was associated with more than a 45% greater risk of fatal and non-fatal coronary heart disease (risk ratio [RR]: 1.48) and a 15% greater risk of stroke (RR: 1.15), rather than total cardiovascular disease or heart attack, as stated in the book. This will be revised in the next edition of the book.
Section Summary: Epidemiological studies have consistently reported that short sleep (and long sleep) is associated with a significantly higher risk of features of cardiovascular and cerebrovascular disease. Corrections will be made in the next edition of the book revising participant study numbers and cardiovascular features examined.
§ § §
Has the World Health Organization indicated that nighttime shift work is a probable carcinogen?
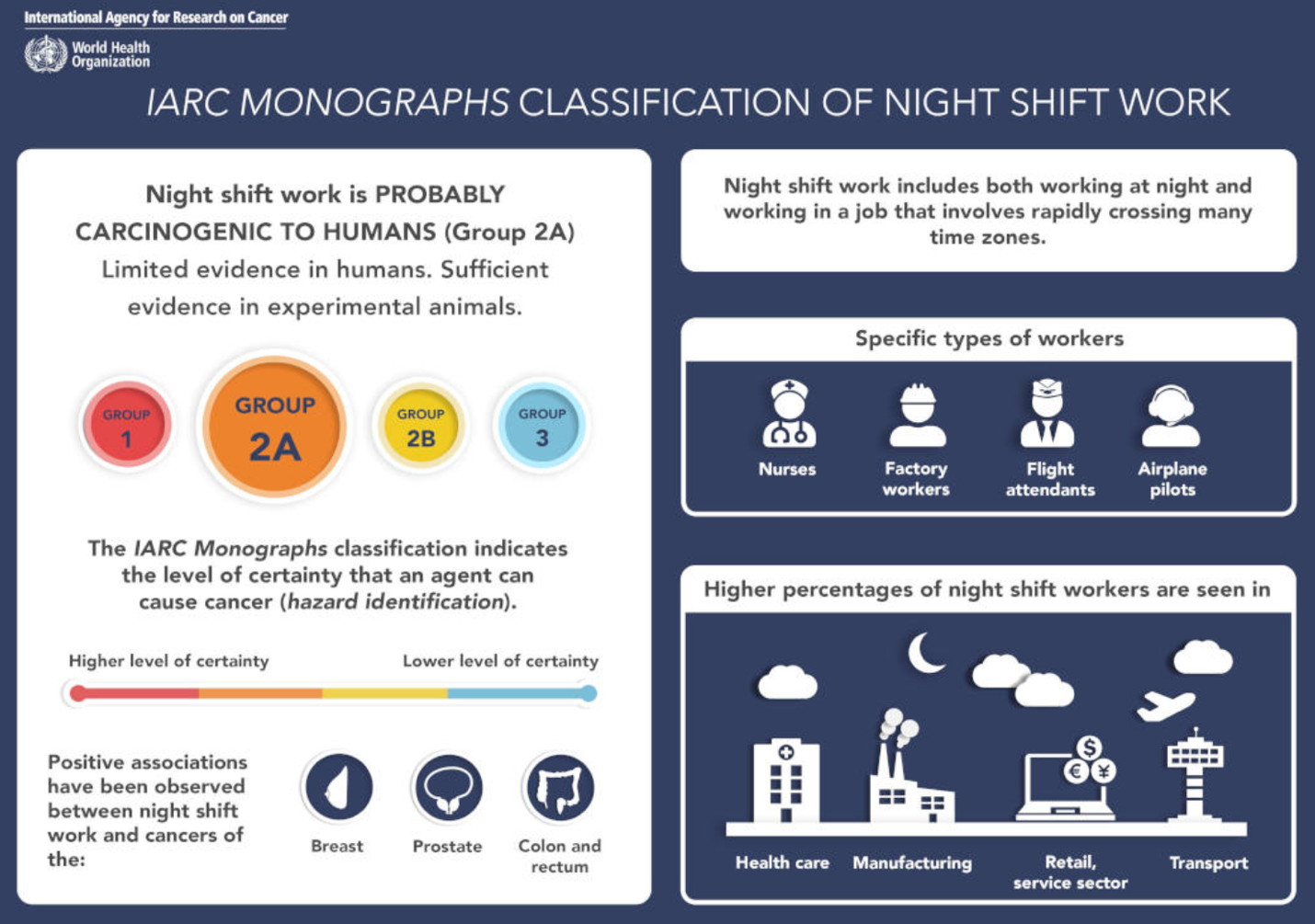
In 2007 the International Agency for Research on Cancer (IARC) of the World Health Organization (WHO) classified nighttime shift work as a probable carcinogen to humans. In 2019, incorporating newly-reviewed data since that time, they upheld the classification.
To resolve any confusion that some readers have had, future editions of the book will be clear that the IARC is part of the WHO.
Section Summary: Nighttime shift work is currently classified by the WHO with the label of a Class 2A carcinogen— “probably carcinogenic to humans.”
§ § §
Living creatures and the generation of a natural circadian cycle.
Most living creatures express a circadian rhythm, but there are exceptions. For example, certain mammals when in a torpor state underground can show an absence of circadian rhythmicity measured in body temperature or by gene activity. Another example is in specific birds during the migration period, where circadian rhythms weaken, although they do not entirely stop.
Section Summary: A correction for future editions of the book will therefore read, “Most living creatures on the planet…”, not “Every living creature…”.
§ § §
Sleep indications from the Centers for Disease Control (CDC), the World Health Organization (WHO), and sleep loss as a public health epidemic.
The Centers for Disease Control (CDC) has stated that, “Insufficient sleep is a public health epidemic.”
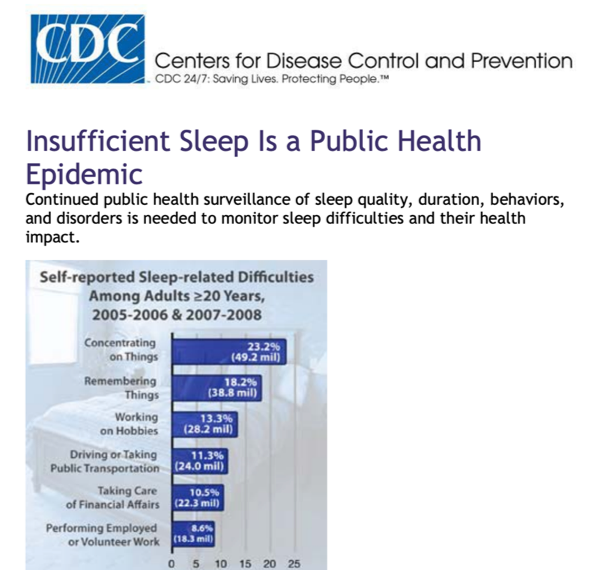
The CDC indicates a minimum 7 hour sleep duration (per 24) for adults. The recommendation is that adults need 7 hours of sleep or more.
The book’s misattribution of the CDC statement to the WHO will be corrected in the next edition.
Based on data regarding sleep difficulties, WHO researchers have described the health dangers of inadequate sleep. Dr. Valery Gafarov, a lead researcher at the WHO exploring cardiovascular disease, has stated:
“Sleep is not a trivial issue. In our study it was associated with double the risk of a heart attack and up to four times the risk of stroke. … Guidelines should add sleep as a risk factor to recommendations for preventing cardiovascular disease”
Section Summary: The CDC, not the WHO, has classified insufficient sleep as a public health epidemic. Both organizations have stated that inadequate and disrupted sleep is dangerous for human health.
§ § §
Does every species studied to date sleep, and does sleep serve a vital function?
Sleep researchers Cirelli and Tononi conducted an in-depth review of the presence of sleep across all animal species. In the course of this review, they examined the hypothesis that sleep is not universal (a view originally proposed by one scientist, and also see p.38, that some readers have noted).
After comprehensively evaluating the evidence, Cirelli and Tononi found precisely the opposite. In refuting this hypothesis, Cirelli and Tononi stated:
“By reviewing the data used to support the claim that sleep is not universal, we instead reach the opposite conclusion: sleep is present and strictly regulated in all animal species that have been carefully studied so far.”
The book states that sleep has been found in “Every species studied to date…” This will be revised to, “Every animal species studied to date…”.
As to the vital function of sleep, Cirelli and Tononi assessed data across species, including those species in which the presence of sleep has been called into question: dolphins, bullfrogs, white-crowned sparrows, coral reef fish, tilapia, perch, zebrafish, cockroaches and honey bees.
Following this evaluation, they arrived at a conclusion similar to that of the book:
“[t]here is no convincing case of a species that does not sleep, no clear instance of an animal that forgoes sleep without some compensatory mechanism, and no indication that one can truly go without sleep without paying a high price.“
They went on to state:
What many concluded long ago still seems to hold: the case is strong for sleep serving one or more essential functions.”
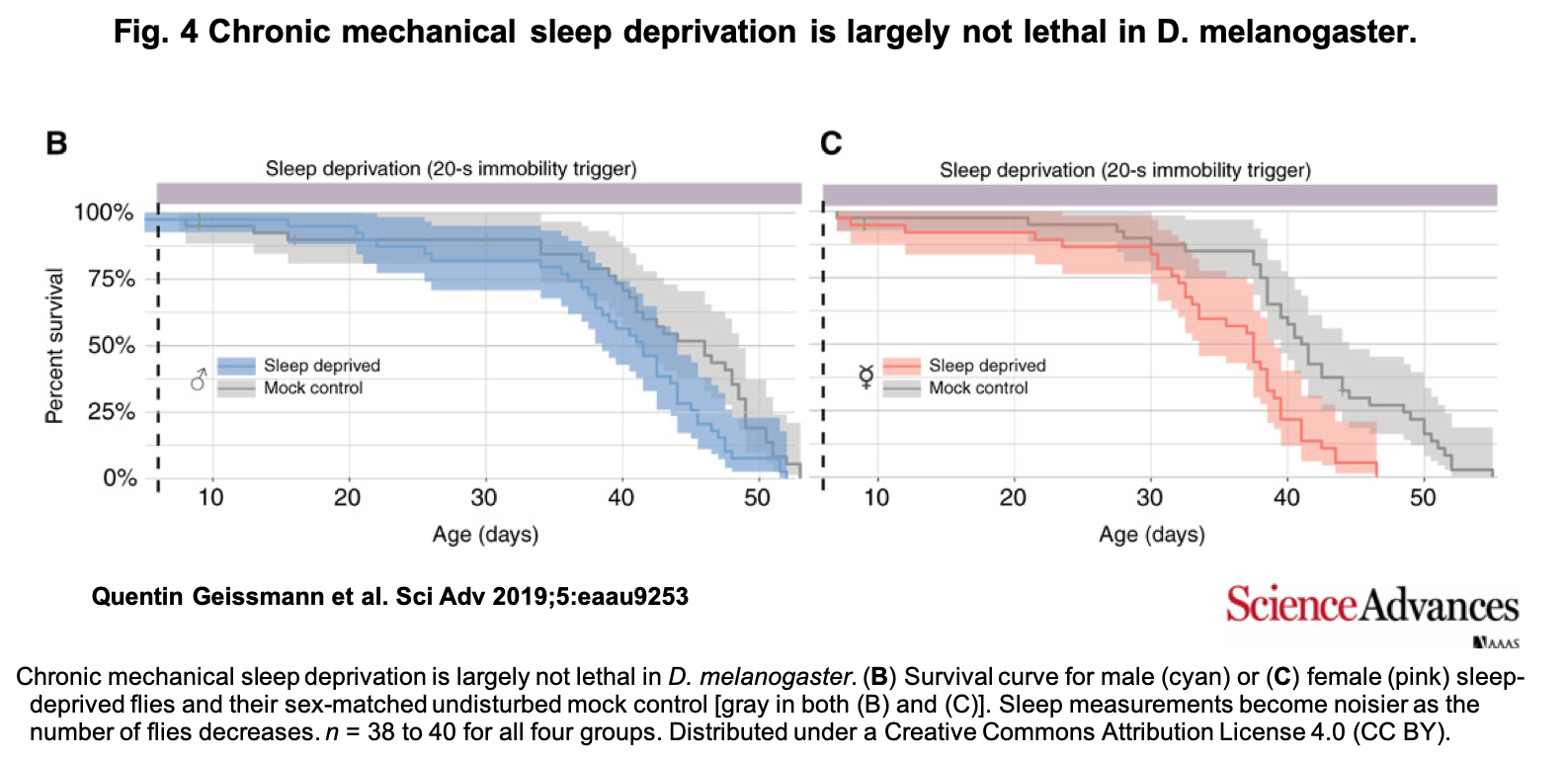
A 2019 publication examining a strain of fruit flies has questioned whether or not sleep is vital. However, the methodology, and thus the validity, of the conclusions of the paper have limitations. For example, the authors of this study developed a new method of scoring sleep using arousal thresholds, which leaves unclear whether or not the scientists were measuring flies at rest (quiescence), or during sleep itself.
Sleep typically needs to be defined on the basis of more than immobility. Indeed, the study and its methods have come under criticism from one of the leading authorities in the field of sleep research:
“I’m not convinced that the micro-movements they report are not part of sleep behavior,’ said Amita Sehgal, a professor at the University of Pennsylvania who pioneered the study of sleep in flies. If that is the case, the flies may have been able to sleep more than researchers realized.”
The statistical power of the study also has limitations. If one looks at the survival curves, there are evidential trends towards the sleep-deprivation and sleep-rested (control) groups differing in their survival rates (figure below: panels B and C, comparing grey survival curves of the control flies to the blue and pink survival curves of the sleep-deprived flies).
This is relevant because the key experimental groups in these mortality analyses only contained 38-40 flies. Replication with several hundred flies may offer a more robust test of the hypothesis that sleep deprivation is lethal in this strain of fruit flies.
Section Summary: The weight of evidence continues to support the original conclusion: sleep appears to be universal, present in every animal species carefully studied so far, and serves one or more vital functions.
§ § §
Sleep and injury risk
The book described a research study that examined injury risk in adolescent athletes on the basis of total hours of sleep per night. The study included 112 individuals.
As shown in the original study, as the athletes’ sleep amount progressively decreased from 9 to 6 hours, injury risk increased. This was depicted in a graphic in the book. The study also reported a group of individuals getting 5 hours of sleep a night. This group’s injury risk was also high, though lower than the adjacent 6-hour group. However, noted by the authors in communication, the 5 hour group was of a size small enough to challenge robust estimate of injury risk, and was not represented in the book’s graphic. Related, the authors averaged the data for statistical power, comparing those getting less than 8-hours with those getting more than this amount.
To counter any confusion, including power issues at either end of the sleep duration distribution, and to better represent the statistical analysis of the study authors, future editions of the book will include a new graphic. This figure will depict the pooled injury risk of those getting less than 8 hours of sleep, relative to those getting 8 hours or more.
Furthermore, the revised edition of the book will note a new 2019 meta-analysis that confirms this original result. Here, less sleep (and worse quality of sleep) was associated with greater injury risk, reflected in the authors’ conclusion:
“Our results thus suggest that adolescents who either chronically sleep less than 8 hours per night, or have frequent night time awakenings, are more likely to experience sports or musculoskeletal injuries.“
§ § §
Miscellany
There were several values in the book where percent changes required updating regarding their negative amount (which cannot exceed 100 percent reduction), and will be revised in the next edition. This includes discussion of changes in electrical brainwave activity in infants of alcoholic mothers in Chapter 5, of gene expression following sleep loss in Chapter 8, and of medical diagnostic rates in Chapter 15.
§ § §
Why We Sleep and readers who are anxious about sleep and/or struggling with sleep.
For the same reason it is important that books are published on the dangers of substance use or obesity or stress, and that organizations like the CDC and WHO publish health advisory documents for public consumption, I believe in the importance of making information on sleep available to the general public.
There is, however, a collection of people who struggle with sleep and are most anxious about it. For those individuals, their anxiety may very understandably increase when reading about the impact of insufficient sleep, including information contained in the book [17].
In addressing this important issue, first, a cautionary note to such effect will be added in future editions of the book, helping alert the reader to this possibility, and thus allowing for individual discretion on this matter.
Second, a revised preface of the book will advise that it is best to maintain a balanced appreciation for the importance of sleep, as rumination about lost sleep in nights past can be counterproductive. The book’s advice will be directed towards a focus on nights ahead, aided by the recommendations given by sleep medicine for improving sleep.
Third, the book will add directions and resources for help with sleep difficulties beyond those it already includes [18].
§ § §
Footnotes:
[1] It is interesting to note that even in the 8-hour sleep group, there was a trend towards gradual impairment over time. Possible explanations include boredom in doing the task for so many days in a row, and/or the fact that even 8 hours a night is insufficient to maintain optimal performance. The latter is supported by a sister study showing no such neurocognitive performance deterioration over a week in individuals provided with a 9-hour sleep opportunity each night.
[2] Fitting the genetic, physiological and neurocognitive findings, short sleep has also been associated with a worse quality of life. A 2014 Gallup poll in 7,058 U.S. adults examined the relationship between sleep duration and global well-being, a measure that combines five wellness categories: Physical, Financial, Purpose, Social and Community. Highest levels of well-being were reported in people sleeping 8 hours a night (figure below). Sleeping 6 hours a night was associated with a >5-point decline in well-being, relative to those sleeping 8 hours a night .

[3] Additional risk factors influencing the association between long sleep and mortality may also include depression, low socioeconomic status and poor general health, including undiagnosed chronic comorbid conditions, as well as physical inactivity.
[4] An example is poor quality sleep associated with sleep apnea. Sleep apnea is rarely measured in epidemiological studies, yet sleep apnea is significantly associated with greater mortality risk. Thus, other conditions, morbidities and behaviors (e.g., sleep apnea, depression, chronic pain, alcohol use) can underlie extended sleep duration and thus lead to an association with higher risk of death.
[5] Beyond lifestyle changes (e.g. family, retirement) that may impact sleep duration, the simple factor of aging will significantly change an individual’s sleep amount and sleep quality over time.
[6] If you are a healthy adult who has a high sleep need and become worried by these associations with long sleep, appreciating the concept of sleep efficiency is critical. Assuming you have a healthy sleep efficiency (85%), to sleep 9 hours in terms of duration (i.e. to be a long-sleeper), you would need to be consistently in bed for 10 hours and 36 minutes a night.
[7] Studies:
[8] The risk-value after taking into account age, examination years, cumulative smoking history, family cancer history, and depression (HR: 2.12). The risk was still almost double (HR: 1.96) when additionally controlling for alcohol consumption, physical activity, body mass index, marital status, education years, night work, employment status, asthma and chronic bronchitis.
[9] Regarding the lack of responsivity to sleeping medications (called, “hypnotics”) in patients with FFI (i.e. patients are refractory or resistant to medications), Kaufman and colleagues have stated: “Fatal familial insomnia (FFI) consists of progressively severe insomnia, refractory to hypnotics”. This is similar to the statement regarding treatment in FFI patients by Sundstrom and Dreher: “There is no known procedure or treatment for delaying the onset of symptoms or modifying the disease course.”
[10] de Manacéïne M. Quelques observations expérimentales sur I’influence de I’insomnie absolue. Arch. Ital. Biol. 1894;21:322-5.
[11] Translation by Bentivoglio & Grassi-Zucconi
[12] Daddi r. Sulk alterazioni degli elementi del sistema nervosa centrale nell’insonnia sperimentale. Rivista di Patologia Nervasa e Mentale 1898;3:1-12. Tarozzi G. Sull’influenza dell’insonnio sperimentale sui ricambio materiale. Rivista di Patologia Nervosa e Mentale 1899;4: 1-23. Daddi L. Sulle alterazioni del sistema nervoso centrale nella inanizione. Rivista di Patologia Nervosa e Mentale 1898;3:295- 300.
[13] Translation by Bentivoglio & Grassi-Zucconi
[14] In the Pittsburgh Sleep Quality Index (PSQI), a well-validated instrument for assessing sleep quality, habitual sleep efficiency >85% is normative (p.212), as indicated by the scoring of 0 for those who have this efficiency level or above.
[15] Note, however (and as stated in Chapter 14 of the book), this is not to suggest that remaining in bed awake for long, continuous periods of time is advised. Such longer periods of time awake can lead to conditioning, where the brain learns an association between the bed and consistently being awake. One of the principles of cognitive behavioural therapy for insomnia (CBT-I) is not to remain awake in bed for longer than 20-25 minutes (also noted in the book’s Appendix concerning sleep tips, #12). Instead, CBT-I practices suggest getting out of bed, and returning when sleepy. The notion being that a person then gradually re-learns the positive association between the bed and being asleep, helping restore confidence in an individual’s ability to be able to sleep in bed.
[16] Similar advocacy regarding the dangers of drowsy driving has been made by the director of the Division of Sleep Medicine at Harvard Medical School, Dr. Charles A.Czeisler:
“Although some contrarians continue to argue that health concerns about sleep deficiency are overrated, the fact that an estimated 58.8 million of America’s licensed drivers report driving while drowsy each month and that 7.5 million of them lose that struggle and fall asleep at the wheel each month, causing more than 50,000 debilitating injuries and 64,00 traffic fatalities annually, demonstrates that many Americans are not even obtaining the sleep that they need to conduct routine daily functions like driving, let alone maintain optimal mental and physical fitness. Compelling evidence thus reveals that sleep is vital for both the brain and the body. For this reason, the National Sleep Foundation has launched Sleep Health, a new journal dedicated to ensuring that research addressing the broader public health implications of the epidemic of sleep deficiency has a permanent home.”
[17] On a personal note, I can sympathize with this position. As a person who struggles with anxiety, I read Robert Sapolsky’s seminal book, Why Zebras Don’t Get Ulcers. The book details the collection of deleterious consequences of stress and high anxiety. The knowledge I gained from Sapolsky’s book did increase my own anxiety. Yet the book’s content motivated me to make lifestyle changes that ultimately lowered my physiological stress and improved my general health. Still, I very much appreciate that this may not be true for others regarding information about sleep.
[18] For example, National Public Radio in the US aired a meaningful segment on the issue of sleep difficulties, sleep worry and insomnia. They offered tips that are consistent with those provided by healthcare services, and those provided in the books’ Appendix. These were (in paraphrase):
- Write down your anxious thoughts; then replace them with more rational thoughts.
- Develop relaxation techniques: Lots of smartphone apps can help, like Headspace, Calm, 10% Happier, Insight Timer.
- The bedroom is only for sleep (and sex); no electronic devices, no lying in bed, ruminating.
- Log your sleep time to get a reality check on how much you’re actually sleeping.
- Restrict the amount of time you spend in bed based on information from your sleep log. Cutting back on time spent in bed can mean spending more time in bed actually sleeping.

You must be logged in to post a comment.